IntroductionIntroducciónالمقدمة
Subacromial impingement syndrome (SIS) represents the most common cause of shoulder pain, accounting for approximately 36% of all shoulder pathologies [1,2]. SIS refers to pain and functional limitation associated with structures within the subacromial space [1,2]. Contemporary literature increasingly favours the term “subacromial pain syndrome” (SAPS) to reflect the multifactorial and often non-structural nature of this condition; however, the term SIS is retained in this study for consistency with the diagnostic framework used during participant selection [3].
A primary extrinsic contributor to SIS is altered scapulothoracic rhythm [2]. Scapular upward rotation contributes approximately 30–40% of scapulohumeral rhythm, and reductions in this motion are strongly associated with various shoulder pathologies [4]. Effective treatment strategies should focus on assessing and correcting scapular positioning and restoring optimal scapulohumeral mechanics [2,4].
Mobilization with movement (MWM) differs from traditional passive joint mobilization techniques in that it incorporates active patient movement during the application of the mobilization [10–14]. MWM has demonstrated superior immediate effects on pain reduction and range of motion compared to passive and sham techniques in peripheral joint conditions [10–14]. However, limited evidence exists evaluating the duration of these effects and the potential additive benefits when combined with neuromuscular reeducation strategies [11,13].
Purpose: To evaluate the effects of a single session of MWM alone compared with MWM combined with neuromuscular reeducation exercise on pain, active shoulder flexion range of motion (AROM), and the duration of these outcomes in recreational athletes with subacromial impingement syndrome.
MethodsMétodosالمنهجية
2.1Study Design
This quasi-experimental intervention utilised an ABAC single-subject withdrawal design across four participants, with each participant serving as their own control. Ethical approval was obtained from the Concordia University Wisconsin Institutional Review Board (IRB #1602982-1). All participants provided written informed consent prior to participation.
2.2Participants
Four recreational athletes (2 males, 2 females; ages 19–21) diagnosed with SIS were recruited from Concordia University Wisconsin. A recreational athlete was defined as an individual who participates in athletics at a recreational level, trains 1–4 times per week, and does not exceed eight hours per week in a single activity [16].
| Participant | Age | Gender | Height | Weight (lbs) | Involved Arm |
|---|---|---|---|---|---|
| 1 | 20 | Male | 5'0" | 123 | Right |
| 2 | 21 | Female | 5'7" | 155 | Left |
| 3 | 19 | Female | 5'7" | 145 | Right |
| 4 | 19 | Male | 6'1" | 178 | Left |
| Mean | 19.75 | 50% Male | 5'6" | 150.25 | 50% Right |
2.3Selection Criteria
Participants were included if they were cleared for physical activity and scored between 5 and 10 on the Tegner Activity Level Scale. Exclusion criteria included: upper extremity or cervical spine surgery within the past year; prior diagnosis of adhesive capsulitis, grade III rotator cuff tear, biceps tendon tear, labral tear, or hooked acromion; upper extremity fracture within the past year; history of systemic or neurological disorders, cervical radiculopathy, cancer, active inflammatory disease, or neuromuscular disorders; and presence of numbness or tingling in the upper extremity.
Eligible participants underwent clinical screening using an orthopedic test cluster for SIS: Hawkins-Kennedy Test, Neer’s Sign, Empty Can Test, Painful Arc Sign, and External Rotation Resistance test (sensitivity 0.75; specificity 0.74; ≥3 positive tests required) [17].
2.4Outcome Measures
Active Shoulder Flexion AROM: Measured using an Acumar digital inclinometer (ICC = 0.90–0.98) [19,20]. Participants positioned standing; inclinometer at midpoint of humeral shaft. Instruction: “Stand upright, position your thumb toward the ceiling, and raise your arm forward as far as possible without reaching pain.”
Global Rating of Change Scale (GROC): 15-point self-reported pain scale; MCID ≥5 points [21]. Administered immediately post-intervention and at 24-hour follow-up.
2.5Study Timeline
| Phase | Duration | Procedures |
|---|---|---|
| Baseline A1 | ≥5 days | Demographic data, clinical screening, informed consent, baseline AROM measurements |
| Intervention B | 1 day | MWM alone; GROC scale; AROM measured every minute × 30 min |
| Baseline A2 | ≥5 days | 24-hour post-intervention GROC; baseline AROM measurements |
| Intervention C | 1 day | MWM + neuromuscular reeducation; GROC scale; AROM every minute × 30 min |
| Follow-Up | 1 day | 24-hour post-intervention GROC and AROM measurements |
2.6Interventions
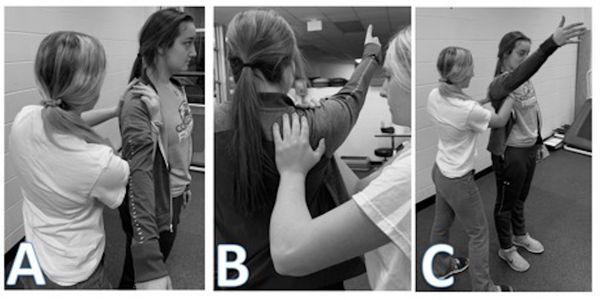
Intervention B — MWM Alone (45 min): MWM performed using clinician-applied posterior-to-anterior scapular fixation (Figure 1). Active glenohumeral flexion; 4/2/2 tempo at 60 BPM; 3 sets × 20 repetitions; 30 s rest between sets. Post-intervention: GROC reassessed; AROM recorded every minute for 30 minutes.
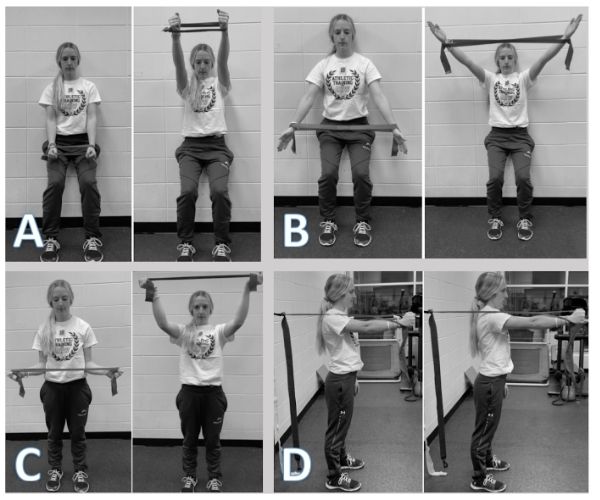
Intervention C — MWM + Neuromuscular Reeducation (75 min): Identical MWM protocol as Phase B, followed immediately by neuromuscular reeducation exercises targeting the serratus anterior, pectoralis major/minor, and upper/lower trapezius (Figure 2) [25–27]:
- Forward flexion with horizontal abduction (130°)
- Scaption with horizontal abduction (130°)
- Elevation with external rotation (90°)
- Serratus punch (shoulder protraction)
Protocol: 3 sets × 10 repetitions per exercise; 60 s rest between sets; 4/2/2 tempo at 60 BPM; red resistance band [28].
2.7Statistical Analysis
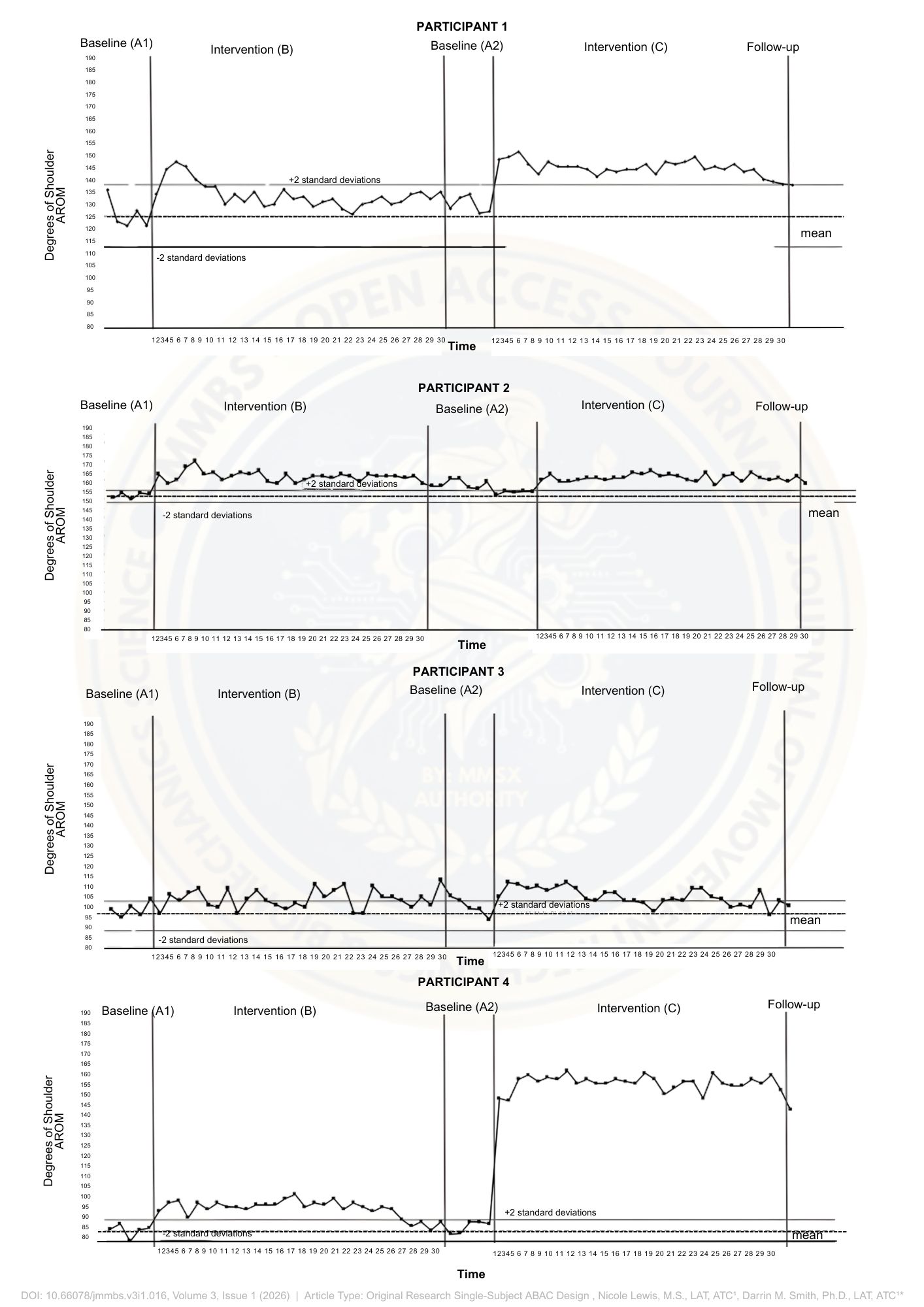
Two-band standard deviation method [30]. Significance: two consecutive data points outside upper/lower two-SD bands. “Return to baseline”: two consecutive AROM measurements within baseline SD range. SD values: Participant 1: ±12.15°; Participant 2: ±3.15°; Participant 3: ±7.05°; Participant 4: ±5.95°.
ResultsResultadosالنتائج
Nine participants were initially recruited; three did not meet inclusion criteria; two withdrew due to external conflicts. Four participants completed the study and were included in the final analysis.
3.1GROC Results
Clinically meaningful improvements in pain (MCID ≥5 points) were observed in Participant 1 following MWM alone, and in Participants 1 and 4 following the combined intervention. At 24-hour follow-up, sustained improvement was observed only in Participant 4 following the combined intervention.
| Participant | Post-MWM Alone | 24h Post-MWM Alone | Post-MWM + Exercise | 24h Post-MWM + Exercise |
|---|---|---|---|---|
| 1 | 5* | 2 | 5* | 4 |
| 2 | 2 | 1 | 2 | −1 |
| 3 | 2 | 2 | 3 | 2 |
| 4 | 4 | 0 | 6* | 5* |
3.2AROM Results
Statistically significant increases in AROM were observed in Participants 1, 2, and 4 following both intervention conditions. The MWM-plus-exercise condition produced greater average increases in AROM (23.2°) compared to MWM alone (8.4°), along with longer-lasting effects (mean duration: 25.5 minutes vs. 15 minutes). Participant 3 demonstrated no measurable duration of improvement for either intervention. Participants 2 and 4 maintained improvements beyond 30 minutes, with extended effects observed at the 24-hour follow-up following the combined intervention.
| Measure | Participant 1 | Participant 2 | Participant 3 | Participant 4 |
|---|---|---|---|---|
| Baseline A1 Mean (±SD) | 125.7° (±12.15) | 151.7° (±3.15) | 97.9° (±7.05) | 89° (±5.95) |
| Post-MWM Alone (B) | 134° | 163° | 96° | 98° |
| % Change from A1 | 6.6% | 7.4% | −1.9% | 10.1% |
| Duration (min) | 4 | 30 | 0 | 25 |
| Baseline A2 Mean (±SD) | 129.7° (±12.15) | 156° (±3.15) | 99.2° (±7.05) | 90.6° (±5.95) |
| Post-MWM + Exercise (C) | 148° | 160° | 104° | 151°* |
| % Change from A2 | 14.1% | 2.6% | 4.8% | 66.7% |
| Duration (min) | 30 | 30+ (24h) | 0 | 30+ (24h) |
DiscussionDiscusiónالمناقشة
This study provides novel insight into the standalone and combined effects of MWM and neuromuscular reeducation in recreational athletes with SIS. Both intervention strategies resulted in improvements in pain and range of motion; however, the combined MWM-plus-exercise condition produced superior outcomes in both magnitude and duration. Substantial inter-participant variability was observed, emphasising the importance of individualised treatment strategies.
4.1Patient-Reported Pain
This study represents the first investigation utilising the GROC scale to evaluate the effectiveness of MWM in individuals with SIS. From a mechanistic perspective, MWM may induce hypoalgesic effects through peripheral mechanoreceptor stimulation and modulation of nociceptive input via gate control mechanisms [35]. The incorporation of active movement may facilitate neuromuscular reorganisation and improved proprioceptive mapping, while scapular repositioning may optimise force-couple relationships and reduce subacromial compression [36].
4.2Inter-Participant Variability
Participant 3, who demonstrated minimal response, may have exhibited greater structural contributions to impingement that are less responsive to scapular repositioning strategies. Contributing factors may include baseline differences in scapular mechanics, rotator cuff strength, joint mobility, and psychological variables such as fear-avoidance or pain perception.
4.3Glenohumeral Range of Motion
This study is the first to evaluate the short-term duration of MWM effects on pain-free glenohumeral flexion AROM, and the first to apply a single-subject design to investigate MWM effects in the shoulder. The observed immediate improvements are consistent with previous literature [11,13,37,38].
4.4Comparison of Treatment Strategies
The combined MWM-plus-exercise condition demonstrated superior AROM improvement and duration of effect. With the exception of Participant 2, all participants demonstrated greater improvements following the combined intervention. The observed superiority may be attributed to enhanced neuromuscular activation and improved mechanical alignment. From a mechanical perspective, improved coordination between the rotator cuff and scapular stabilisers may enhance moment arm efficiency (τ = r × F), facilitating more controlled and efficient force transfer throughout the kinetic chain.
4.5Clinical Implications
MWM alone: mean 8.4° AROM increase; approximately 15 minutes duration. MWM + exercise: mean 23.2° increase; approximately 25.5 minutes duration. These findings suggest that the addition of neuromuscular reeducation enhances both the magnitude and persistence of treatment effects. The application of MWM, particularly when combined with neuromuscular reeducation, may contribute to improved force-vector alignment and reduction in aberrant joint loading patterns, thereby decreasing subacromial compressive stress.
4.6Limitations
Limitations include: lack of prior literature on duration of MWM effects in SIS; inability to definitively differentiate primary from secondary impingement without imaging; inability to fully control participant adherence outside the study; and individual variability in physiological and psychological responses.
ConclusionConclusiónالخلاصة
This single-subject ABAC withdrawal study provides scientific support for the use of mobilization with movement (MWM), both as a standalone intervention and in combination with neuromuscular reeducation exercise, in the management of recreational athletes presenting with secondary subacromial impingement syndrome (SIS). The addition of neuromuscular reeducation exercise was associated with greater improvements in both the magnitude and duration of pain reduction and AROM gains. Notable inter-individual variability reinforces the importance of individualised clinical decision-making. Further research with larger sample sizes and controlled study designs is warranted.
Author Biographical Notes
Declarations
IRB #1602982-1, Concordia University Wisconsin. All participants provided written informed consent. Written consent for image publication obtained by PI.
The authors report no competing interests to declare.
No external funding was provided over the duration of this investigation.
Raw minute-by-minute AROM data available from the corresponding author (darrin@colabphysicians.com) upon reasonable request. Also available in Figure 3 and supporting Excel sheets.
References
All references formatted in accordance with APA 7th Edition.
- Steuri R, et al. Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement. Br J Sports Med. 2017;51(18):1340–1347.
- Alqunaee M, Galvin R, Fahey T. Diagnostic accuracy of clinical tests for subacromial impingement syndrome. Arch Phys Med Rehabil. 2012;93(2):229–236.
- Diercks R, et al. Guideline for diagnosis and treatment of subacromial pain syndrome. Acta Orthop. 2014;85(3):314–322.
- Surenkok O, Aytar A, Baltaci G. Acute effects of scapular mobilization in shoulder dysfunction. J Sport Rehabil. 2009;18(4):493–501.
- Starkey C, Brown S. Examination of Orthopedic and Athletic Injuries. 4th ed. F.A. Davis; 2015.
- Michener L, McClure P, Karduna A. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech. 2003;18(5):369–379.
- Harrison A, Flatow E. Subacromial impingement syndrome. J Am Acad Orthop Surg. 2011;19(11):701–708.
- Dorrestijn O, et al. Conservative or surgical treatment for subacromial impingement syndrome? J Shoulder Elbow Surg. 2009;18(4):652–660.
- Senbursa G, Baltaci G, Atay A. Comparison of conservative treatment with and without manual physical therapy for shoulder impingement. Knee Surg Sports Traumatol Arthrosc. 2007;15(7):915–921.
- Stathopoulos N, Dimitriadis Z, Koumantakis G. Effectiveness of Mulligan’s MWM on pain and disability. Physiotherapy. 2019;105(1):1–9.
- Teys P, Bisset L, Vicenzino B. Initial effects of Mulligan’s MWM on range of movement and pressure pain threshold. Man Ther. 2008;13(1):37–42.
- Pourahmadi M, et al. Effectiveness of MWM on low back pain. Clin Rehabil. 2018;32(10):1289–1298.
- Kachingwe A, et al. Comparison of manual therapy techniques with therapeutic exercise in shoulder impingement. J Man Manip Ther. 2008;16(4):238–247.
- Noten S, et al. Efficacy of mobilization techniques in primary adhesive capsulitis. Arch Phys Med Rehabil. 2016;97(5):815–825.
- Moon G, et al. Comparison of Maitland and Kaltenborn mobilization in frozen shoulders. J Phys Ther Sci. 2015;27(5):1391–1395.
- Stirling A, Kerr G. Perfectionism and mood states among recreational and elite athletes. Athl Insight. 2006;8(4):13–27.
- Michener L, et al. Reliability and diagnostic accuracy of 5 tests for subacromial impingement. Arch Phys Med Rehabil. 2009;90(11):1898–1903.
- Ratcliffe E, et al. Subacromial impingement syndrome and scapular orientation: A systematic review. Br J Sports Med. 2014;48(16):1251–1256.
- Dougherty J, Walmsley S, Osmotherly P. Passive range of movement of the shoulder: Reliability of measurement. J Manipulative Physiol Ther. 2015;38(3):218–224.
- Kolber M, Hanney W. Reliability and validity of shoulder mobility measurements using a digital inclinometer. Int J Sports Phys Ther. 2012;7(3):306–313.
- Kamper S, Maher C, Mackay G. Global rating of change scales: a review. J Man Manip Ther. 2009;17(3):163–170.
- Garrison C, Cook C. The GROC poorly correlates with functional measures and is not temporally stable. J Man Manip Ther. 2012;20(4):178–181.
- Kamper S. Global Rating of Change scales. Aust J Physiother. 2009;55(4):289.
- Neuhauser D, Provost L, Bergman B. The meaning of variation to healthcare managers. BMJ Qual Saf. 2011;20(Suppl 1):i36–40.
- Park KM, et al. Effect of isometric horizontal abduction on pectoralis major and serratus anterior EMG. J Electromyogr Kinesiol. 2013;23(2):462–468.
- Castelein B, et al. Scapulothoracic muscle EMG during elevation in the scapular plane. J Orthop Sports Phys Ther. 2016;46(3):184–193.
- Castelein B, et al. Serratus anterior or pectoralis minor during protraction exercises? Man Ther. 2016;(22):158–164.
- Clarke M, Russell A. NASM OPT. 1st ed. National Academy of Sports Medicine Publishers; 2002.
- Portney L, Watkins M. Principles and Practice of Clinical Research. 3rd ed. F.A. Davis; 2009.
- Nourbakhsh M. Statistical analysis of single-subject data: A comparative examination. Phys Ther. 1994;74(8):768–776.
- Jensen M, Braver S, Karoly P. Measurement of clinical pain intensity: comparison of six methods. Pain. 1986;27(1):117–126.
- Bolton J, Wilkinson R. Responsiveness of pain scales in chiropractic patients. J Manipulative Physiol Ther. 1998;21(1):1–7.
- Herr K, et al. Pain intensity assessment in older adults. Clin J Pain. 2004;20(4):207–219.
- Childs J, Piva S, Fritz J. Responsiveness of the numeric pain rating scale in low back pain. Spine. 2005;30(11):1331–1334.
- Vicenzino B, Paungmali A, Teys P. Mulligan’s MWM, positional faults and pain relief. Man Ther. 2007;12(2):98–108.
- Kibler WB, et al. Clinical implications of scapular dyskinesis: 2013 Scapular Summit. Br J Sports Med. 2013;47(14):877–885.
- Delgado-Gil J, et al. Effects of MWM on pain and ROM in unilateral shoulder impingement. J Manipulative Physiol Ther. 2015;38(4):245–252.
- Haider R, et al. Maitland vs. Mulligan’s mobilization in frozen shoulder. Ann King Edw Med Univ. 2014;20(3):257–264.