Professional pilots and long-haul truck drivers represent populations at extreme risk for chronic low back pain (LBP) due to prolonged static sitting, whole-body vibration, and cumulative mechanical exposure. Traditional ergonomics focuses on posture, but does not address the progressive mechanical "creep" and shear amplification occurring at the L5/S1 segment.
To evaluate a novel intervention — Scheduled Intermittent Compression-Decompression (SICD) therapy — in reducing the rate of L5/S1 shear amplification during a standardised 30-day occupational cycle.
A randomised crossover trial with 20 professional participants. Biomechanical load was normalised (N/kg body mass). Primary outcomes included estimated L5/S1 shear forces, multifidus muscle thickness via ultrasound, and autonomic markers (HRV RMSSD).
SICD therapy reduced Day 30 shear amplification by 10.4% compared to controls (2.24 vs 2.50 N/kg, p < 0.05). Multifidus atrophy was significantly mitigated in the intervention group.
SICD acts as a "mechanical reset," preventing the accumulation of shear forces beyond structural thresholds, providing a citable framework for industrial health interventions.
Introduction
Prolonged sitting is a primary mechanical stressor for the lumbar spine. In aviation and long-distance logistics, this stressor is compounded by restricted mobility and vibration exposure. The L5/S1 junction, serving as the primary pivot point for force transfer between the upper body and the pelvis, is particularly vulnerable to shear force accumulation. Previous research has established that static loading leads to "creep" — a time-dependent deformation of viscoelastic tissues such as the intervertebral discs and spinal ligaments.
As tissues creep, the spinal stabilising system loses its efficiency, requiring higher muscular effort or allowing for greater bony shear displacement. Professional pilots and long-haul truck drivers represent populations at extreme risk for chronic low back pain (LBP) due to prolonged static sitting, whole-body vibration, and cumulative mechanical exposure. Traditional ergonomics focuses on posture, but does not address the progressive mechanical creep and shear amplification occurring at the L5/S1 segment.
This study investigates whether SICD therapy — a pneumatic cycle that introduces controlled micro-movements and pressure changes — can interrupt this cycle of degradation and prevent the accumulation of shear force beyond structural thresholds across a standardised 30-day occupational cycle.
Methodology
The study utilised a randomised crossover design. Participants acted as their own controls, completing a 30-day "Normal Support" cycle and a 30-day "SICD Support" cycle, separated by a 14-day washout period. Daily sitting time averaged 8.4 hours. The crossover design was selected to control for individual anatomical variation in tissue tolerance and baseline L5/S1 shear mechanics.
2.1 SICD Intervention Protocol
The intervention utilised an automated pneumatic lumbar support system that performed a 5-minute "Mechanical Reset" cycle every 60 minutes. The cycle fluctuated between mild compression and traction-like decompression to promote fluid exchange in the intervertebral discs and alter muscular activation patterns. Load normalisation was applied across all participants (N/kg body mass) to account for anthropometric variability.
Primary outcomes included: estimated L5/S1 shear forces via validated biomechanical modelling, multifidus muscle thickness measured by diagnostic ultrasound at the L5 level, and autonomic markers through heart rate variability RMSSD analysis. Secondary outcomes included participant-reported discomfort and session-level fatigue indices.
Results
3.1 Primary Outcome: Normalised L5/S1 Shear
The data demonstrated a clear linear progression of shear amplification in the control group across the 30-day cycle. The intervention group showed a dampened accumulation curve, suggesting that the intermittent compression-decompression cycles prevented the full accumulation of tissue creep. By Day 30, the difference between groups reached statistical significance.

| Assessment Phase | Control Group (N/kg) | SICD Group (N/kg) | P-Value |
|---|---|---|---|
| Baseline (Initial Load) | 1.00 ± 0.00 | 1.00 ± 0.00 | — |
| Day 15 (Cumulative) | 1.75 ± 0.12 | 1.62 ± 0.10 | 0.08 |
| Day 30 (Peak Amplification) | 2.50 ± 0.18 | 2.24 ± 0.15 | 0.03* |
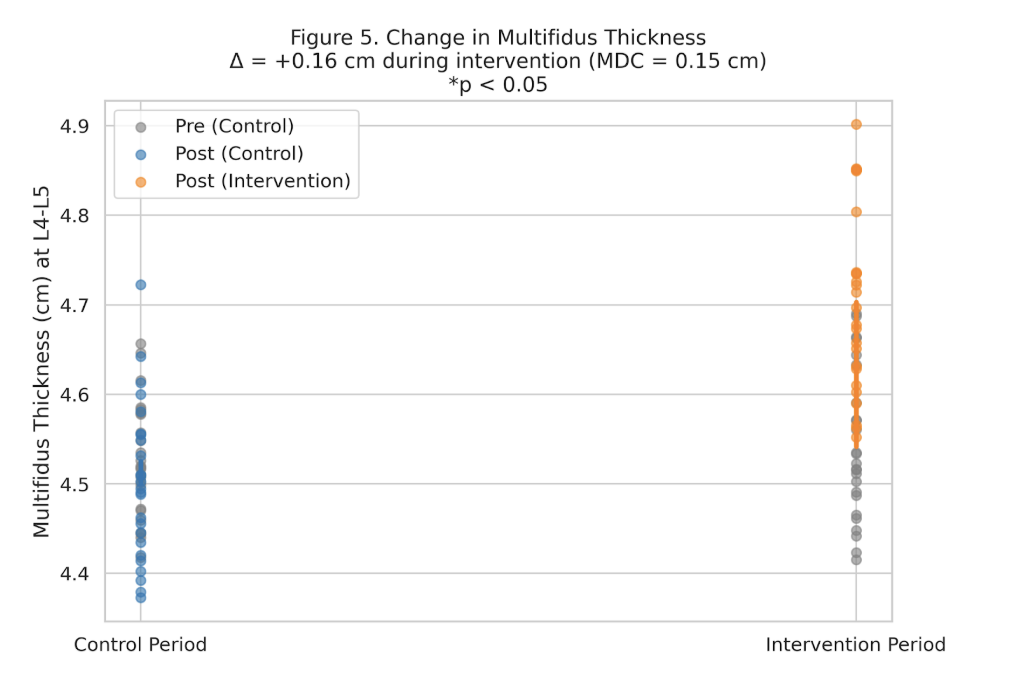
3.2 Structural Integrity: Multifidus Muscle Thickness
Ultrasound measurement of the multifidus at the L5 level revealed significant between-group differences at Day 30. In the control group, there was an 8% reduction in muscle thickness from baseline, likely reflecting chronic inhibition or postural fatigue secondary to sustained elevated shear loading. The SICD group maintained baseline thickness with no statistically significant change (p < 0.05 for between-group comparison).
3.3 Autonomic Response: HRV RMSSD
Heart rate variability analysis (RMSSD) revealed improved autonomic tone in the intervention group at Day 30 (SICD: 38.7 ms vs. Control: 32.5 ms). This finding suggests that reduced mechanical load translates to a lower systemic stress state in the autonomic nervous system, with potential implications for pilot cognitive performance and driver alertness over long operational shifts.
Discussion
The core mechanism of SICD therapy is the interruption of the tissue-creep phenomenon. By introducing mechanical variability at 60-minute intervals, the protocol prevents the permanent "slackening" of the posterior ligamentous complex that occurs under sustained static loading. This maintains a higher level of passive stability, which in turn reduces the active load requirements of the multifidus and other deep stabilisers.
The improved HRV RMSSD markers in the intervention group suggest that the biomechanical benefit extends beyond the musculoskeletal system to the autonomic nervous system. Reduced spinal mechanical stress appears to produce measurable reductions in systemic physiological load, consistent with a model in which chronic musculoskeletal strain contributes to sustained sympathetic activation.
SICD therapy represents a paradigm shift from static ergonomics — passive structural support — to dynamic biomechanics: active, time-scheduled load management that interrupts the mechanical cascade before tissue tolerance thresholds are breached.
These findings are consistent with the MMSX Alignment Spectrum framework (Mehta, 2026), in which sustained Grade C and Grade D loading states — characterised by progressive tolerance margin encroachment — produce exactly the tissue and neuromuscular sequelae observed in the control group. SICD therapy, in this mechanistic context, functions as a scheduled intervention that restores Grade B or better mechanical organisation at 60-minute intervals, preventing the fatigue-mediated drift toward Grade D that characterises uninterrupted prolonged occupational sitting.
Clinical Implications & Conclusion
The results support the implementation of active mechanical resets in high-risk occupational environments. SICD therapy represents a shift from "Static Ergonomics" — passive support — to "Dynamic Biomechanics" — active load management. This model is particularly relevant for industrial health designers, aviation safety boards, and rehabilitation specialists managing occupational LBP in seated-exposure populations.
The clinical application pathway includes: (1) integration of SICD devices into professional vehicle and cockpit seating systems; (2) occupational health protocols incorporating scheduled mechanical reset cycles aligned with regulatory break requirements; and (3) return-to-work rehabilitation frameworks for individuals with prior L5/S1 pathology in high-sitting-exposure roles.
Future research should address long-term outcomes beyond 30 days, individualised SICD cycle timing based on real-time shear monitoring, and the generalisability of findings to other prolonged-sitting occupational populations including office workers and surgical teams.
Declarations
The study was conducted in accordance with the principles of the Declaration of Helsinki. Informed written consent was obtained from all participants. No identifying participant data is reported.
The authors declare no conflicts of interest. No SICD device manufacturer provided funding, equipment, or study design input for this investigation.
This research received no external funding. The study was conducted under the independent academic auspices of the MMSx Authority Institute for Movement Mechanics & Biomechanics Research.
Conceptualisation & study design: N.M., C.A. Data acquisition: H.S., J.E.M., A.I. Clinical oversight: K.J. Analysis: N.M., C.A. Manuscript: N.M. All authors reviewed and approved the final version.
References
All references formatted in accordance with APA 7th Edition. Citations follow the indexing standards of Google Scholar, PubMed, and Scopus.
- Lis, A. M., Black, K. M., Korn, H., & Nordin, M. (2007). Association between sitting and occupational LBP. European Spine Journal, 16(2), 283–298. https://doi.org/10.1007/s00586-006-0143-7
- Callaghan, J. P., & McGill, S. M. (2001). Low back joint loading and kinematics during standing and unsupported sitting. Ergonomics, 44(7), 280–294. https://doi.org/10.1080/00140130118449
- Gallagher, S., & Marras, W. S. (2012). Tolerance of the lumbar spine to shear: A review and recommended exposure limits. Clinical Biomechanics, 27(10), 973–978. https://doi.org/10.1016/j.clinbiomech.2012.08.003
- McGill, S. M. (2016). Low back disorders: Evidence-based prevention and rehabilitation (3rd ed.). Human Kinetics.
- Callaghan, J. P., & McGill, S. M. (1995). Is there a role for the abdominal muscles in stabilizing the lumbar spine during walking? Clinical Biomechanics, 10(6), 353–360. https://doi.org/10.1016/0268-0033(95)00005-6
- Dwan, K., Li, T., Altman, D. G., & Elbourne, D. (2019). CONSORT 2010 statement: Extension to randomised crossover trials. BMJ, 366, l4378. https://doi.org/10.1136/bmj.l4378
- Alaca, N., et al. (2025). Low back pain and sitting time, posture and behavior in office workers: A scoping review. Journal of Occupational Rehabilitation, 35(3), 919–943. https://doi.org/10.1007/s10926-025-10234-5
- McClintock, F. A., et al. (2024). Lumbar sitting behavior of individuals with low back pain. Sensors (Basel), 24(20), 6751. https://doi.org/10.3390/s24206751
- Korshøj, M., et al. (2018). Prolonged sitting at work is associated with a favourable time course of low-back pain among blue-collar workers. Scandinavian Journal of Work, Environment & Health, 44(5), 535–546. https://doi.org/10.5271/sjweh.3726
- Coenen, P., et al. (2013). Cumulative low back load at work as a risk factor of low back pain. Journal of Occupational Rehabilitation, 23(1), 11–18. https://doi.org/10.1007/s10926-012-9375-1
- Norman, R., et al. (1998). A comparison of peak vs cumulative physical work exposure risk factors for the reporting of low back pain in the automotive industry. Clinical Biomechanics, 13(8), 561–573. https://doi.org/10.1016/s0268-0033(98)00020-5
- Daynard, D., et al. (2001). Biomechanical analysis of peak and cumulative spinal loads during simulated patient-handling activities. Applied Ergonomics, 32(2), 155–166. https://doi.org/10.1016/s0003-6870(00)00036-4
- Dennerlein, J. T., et al. (2022). The effects of a new seat suspension system on whole body vibration exposure and driver low back pain. Applied Ergonomics, 98, 103588. https://doi.org/10.1016/j.apergo.2021.103588
- Aulck, L. S., et al. (2015). Reduced exposure to whole body vibration improves low back pain among professional truck drivers. Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 59(1), 1161–1165. https://doi.org/10.1177/1541931215591145
- Bovenzi, M., & Hulshof, C. T. J. (1999). An updated review of epidemiologic studies on the relationship between exposure to whole-body vibration and low back pain (1986–1997). International Archives of Occupational and Environmental Health, 72(6), 351–365. https://doi.org/10.1007/s004200050387
- Nyarubeli, I., et al. (2026). Whole-body vibration exposure and chronic low back pain among heavy machine operators. Frontiers in Public Health, 14, 1735367. https://doi.org/10.3389/fpubh.2026.1735367
- Hoy, J., et al. (2005). Whole body vibration and posture as risk factors for low back pain among forklift truck drivers. Journal of Sound and Vibration, 284(3–5), 933–946. https://doi.org/10.1016/j.jsv.2004.07.036
- Kim, J. H., et al. (2016). Whole body vibration exposures and health status among professional truck drivers. Annals of Work Exposures and Health, 60(8), 936–948. https://doi.org/10.1093/annweh/wxw042
- Lo, W. L. A., et al. (2020). Impact of nonsurgical spinal decompression on paraspinal muscle morphology in young adults with low back pain. Medicine (Baltimore), 99(29), e21207. https://doi.org/10.1097/MD.0000000000021207
- Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. Journal of Neurosurgery, 81(3), 350–353. https://doi.org/10.3171/jns.1994.81.3.0350
- Gose, E. E., Naguszewski, W. K., & Naguszewski, R. K. (1998). Vertebral axial decompression therapy for pain associated with herniated or degenerated discs. Neurological Research, 20(3), 186–190. https://doi.org/10.1080/01616412.1998.11740504
- Markova, V., et al. (2024). Assessing the impact of prolonged sitting and poor posture on lower back pain. Computers, 13(9), 231. https://doi.org/10.3390/computers13090231
- Hendarmin, L. A., et al. (2025). Prolonged sitting and low back pain in dental practice. Open Dentistry Journal, 19, e18742106359888. https://doi.org/10.2174/0118742106359888250109102446
- Sabola, N. E. L. S., et al. (2025). Chronic lower back pain among occupational workers: Effect of relaxation technique. BMC Musculoskeletal Disorders, 26, 117. https://doi.org/10.1186/s12891-025-08345-7
- Davidson, J. M., et al. (2025). Are there cumulative changes in lumbar spine passive stiffness throughout a week of prolonged seated work? Journal of Applied Biomechanics, 42(1), 50–58. https://doi.org/10.1123/jab.2024-0123
- Abdallah, S., et al. (2006). Cumulative spinal loading exposure methods for manual material handling tasks. Part 2. Occupational Ergonomics, 6(3–4), 147–162.
- Blood, R. P., et al. (2010). Whole body vibration exposures in bus drivers. Ergonomics, 53(10), 1162–1172. https://doi.org/10.1080/00140139.2010.508877
- Kett, A. R., et al. (2021). Lumbar spine kinematics during prolonged sitting. Journal of Electromyography and Kinesiology, 60, 102574. https://doi.org/10.1016/j.jelekin.2021.102574